Laurie's Blogs.

Aug 2017
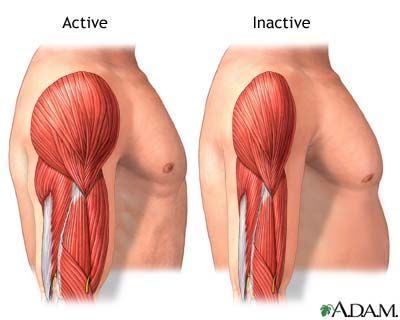
Weakness versus Muscle Inhibition
This from another one of the Mike Reinhold podcasts:
What is the difference between an Inhibited muscle vs a weak muscle?
Inhibited: A muscle that is ‘down regulated’ due to an injury. Pain, inflammation, swelling in a muscle or joint can inhibit muscles from contracting. For example, my son’s vastus medialis muscle is inhibited due to the swelling that is still in his knee subsequent to his ACL reconstruction.
Weak: An inability to produce force and inability to lift a load. For example, because of my appendectomy in early July, I have not exercised much at all. All of my muscles are weaker. I can still use them, they just aren’t as strong.
But then what’s more interesting is what do you do in each scenario?
So, the easiest thing to talk about first, is weakness. Weakness can be combatted by exercise. Any exercise! Use the muscle, push the muscle, make it contract with force. For a deconditioned patient, this could be as simple as short walks on flat terrain. For an athlete, this this can be hill climbing, destination jumping, specific exercises, vigorous swimming or trotting in an UWT. For me, I need to get into the habit again of going to the gym and lifting weights!
An inhibited muscle is trickier. In an acute injury, the inhibition is there to protect the joint. (i.e. in an acute muscle tear, an acute cruciate ligament tear, a post-operative joint, etc.) In these scenarios, you don’t treat the muscle inhibition (right away), you treat the injury, the pain, the inflammation, and the swelling. Where it gets tricky is when inhibition lasts longer than what’s useful. So, in the example of the ACL tear (or post-op ACL reconstruction), after the initial inflammation phase (let’s say 1 week to 10 days), then we may need to help the body ‘remember’ the job of the inhibited muscle. I have found that the e-stim works best for this. Put it on the Quads (and in people, specifically the vastus medialis) and fire it up and have the patient work with it! That last part is so important. You won’t resolve inhibition or strengthen a muscle if the patient isn’t working WITH the e-stim. In other words, you can’t just lie the dog down, strap on the e-stim, and expect him/her to have a stronger muscle afterwards. In dogs, I do a 3-leg stand (lifting the unaffected limb off the ground when the unit is ‘on’). In people, I get them to do a mini-squat while the machine is ‘on’.
The other thing you can’t ignore with an inhibited muscle is inflammation, pain, or swelling. Some of your treatment time must be geared to dealing with these things if they are contributing to the muscle inhibition. That can be addressed with modalities, manual therapy, perhaps a pain medication.
Muscle inhibition is why you won’t get a dog fully rehabbed from an injury or post-operative orthopaedic surgery by just throwing him in the UWT or Pool. They need specific exercises and rehab to address the inhibition. That’s why understanding the difference between inhibition and weakness is a pretty important concept.